
Do I Really Need to Take the Glucose Tolerance Test While Pregnant?

Find out who needs to take the glucose tolerance test during pregnancy and what the results of the glucose test mean.
The oral glucose tolerance test helps to diagnose women who have developed diabetes during pregnancy (gestational diabetes). Most pregnant women will take the test right before the third-trimester begins (somewhere between 24 and 28 weeks).
As a nurse at a community health center, one of my favorite parts of my job is patient education. I love being able to explain things to my patients in ways that help them understand and manage their health better.
I do a lot of education on self-management of diabetes. Most of my patients have a diagnosis of type 2 diabetes but we also see people with type 1 diabetes and pregnant women who have been diagnosed with gestational diabetes.
Thinking that you may have gestational diabetes can be frightening for pregnant women but identifying and treating the disease will reduce the risk of complications.

DISCLAIMER: The information on the site is for informational and educational purposes only. Nothing on the site should be considered medical advice. Always consult your own or your child’s health care provider before acting on any information or recommendations. You can read my full Disclaimer Policy here.
Why Do Women Get Gestational Diabetes?
The simple explanation of diabetes is that the body cannot metabolize glucose (or sugar) properly.
When we eat food, especially carbohydrates, our bodies turn that food into glucose. Our cells need glucose for energy.
Insulin, a hormone produced by the pancreas, acts as a key that opens the door of a cell to allow the glucose to get in.
When someone has diabetes, the insulin is either not working effectively or the body is not making enough insulin. The glucose can’t get into the cells correctly. It then builds up in the blood, leading to high blood glucose levels.
During pregnancy, the placenta secretes hormones in order to supply the fetus with nutrients. Some of these hormones act as “anti-insulin” agents which can cause insulin resistance.
Basically, the hormones produced by your placenta can make your body resistant to your own insulin.
This leads to a pregnant woman’s body requiring MORE insulin than it does when not pregnant in order to appropriately metabolize glucose.
Most women will produce more insulin to compensate for these changes. Some women are unable to make enough extra insulin, which leads to gestational diabetes.
Identifying and treating gestational diabetes can significantly reduce the risk of complications.
What Are the Complications of Gestational Diabetes?
Some of the complications of gestational diabetes include:
- an increased risk of preeclampsia
- a large baby
- high amniotic fluid levels
- low blood sugar in the baby after delivery
- hyperbilirubinemia or jaundice
- neonatal respiratory problems
What To Expect From The Glucose Tolerance Test During Pregnancy

The U.S. Preventive Services Task Force recommends asymptomatic pregnant women get screened after 24 weeks gestation. Pregnant women will generally take the glucose test between their 24th and 28th weeks of pregnancy.
Most of the time, the test is done using a two-step approach.
The first step is the one-hour glucose test.
A pregnant woman who screens positive on the one-hour test (aka who “fails” the test) will have to do the three-hour glucose test.
The one-hour test identifies pregnant women at an increased risk for gestational diabetes.
It doesn’t necessarily diagnose the disease which is why you have to have a follow-up test.
The one-hour test is more practical for most women. It can be performed at any time of day, you don’t need to be fasting, and you don’t need to wait at the lab for 3 hours!
The three-hour test is then used to make a definitive diagnosis.
The three-hour test is more complicated and more costly. This is why it is not used for everyone as a first step approach.
Some OB/GYN practices may use a one-step approach instead of the two different tests (discussed below). However, the American College of Obstetricians and Gynecologists (ACOG) recommends the two-step approach.
The following chart may help explain what to expect during the glucose tolerance test depending on whether your doctor uses the two-step or one-step approach.
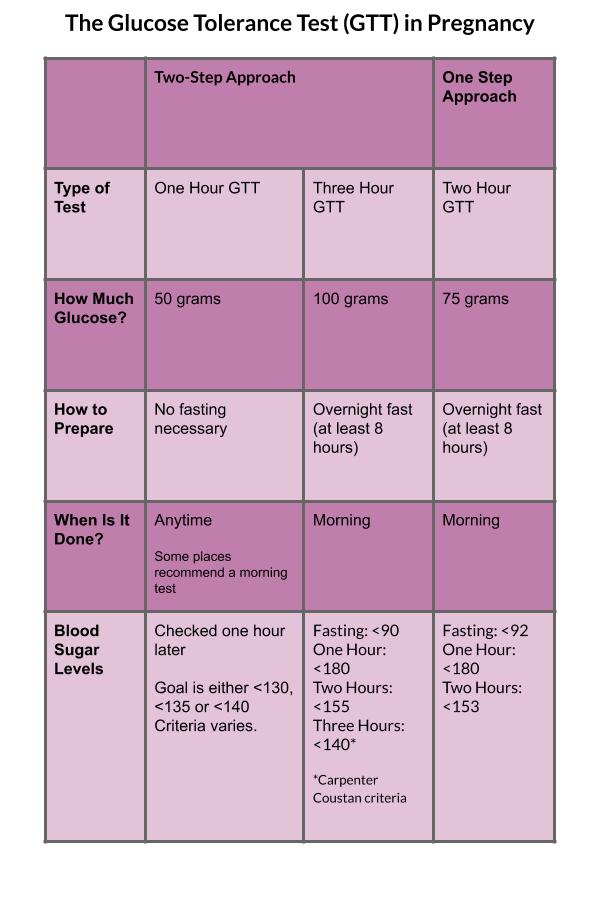
One-Hour Glucose Test
For this test, a pregnant woman will consume 50 grams of oral glucose. This is usually in the form of a drink called Glucola.
The Glucola drink comes in multiple different flavors.
In general, you do not need to fast and the time since the last meal doesn’t matter. Some OB/GYN practices, however, will give stricter instructions.
During my first pregnancy, I did the glucose tolerance test in the afternoon with no regard to what I had eaten that day. With my second pregnancy, my new OB/GYN preferred to have patients test in the morning after eating a protein breakfast. They also instructed me to avoid fruit and juice.
You should try to consume the drink in about 5-10 minutes and note the time you finish it. A blood draw will measure the glucose concentration in your blood one hour later.
In general, if your blood glucose level is greater than 130 mg/dL, you will need to do the three-hour glucose tolerance test (GTT). The cut-off number differs, however, based on the criteria your OB/GYN practice is following. Some providers will only recommend the three-hour GTT if your blood glucose is greater than 135 or greater than 140 after one hour.
You may hear the one-hour test also referred to as a glucose screen, glucose challenge test, or glucose loading test.
Three-Hour Glucose Test
The three-hour test uses 100 grams of oral glucose. Your blood glucose level is checked BEFORE the drink (fasting) and again one hour, two hours, and three hours after finishing.
Traditionally, TWO elevated numbers indicate gestational diabetes. However, ACOG recently noted that just one elevated value can diagnose gestational diabetes (1).
There are two sets of values that your OB/GYN office may use to diagnose gestational diabetes using the three-hour GTT. They may follow either the Carpenter Coustan criteria or National Diabetes Data Group criteria.
Per the Carpenter Coustan criteria, your blood glucose levels should be:
- Fasting: less than 95 mg/dL
- 1 hour after: less than 180 mg/dL
- 2 hours after: less than 155 mg/dL
- 3 hours after: less than 140 mg/dL
Per the National Diabetes Data Group criteria, your blood glucose levels should be:
- Fasting: less than 105 mg/dL
- 1 hour after: less than 190 mg/dL
- 2 hours after: less than 165 mg/dL
- 3 hours after: less than 145 mg/dL
Read next: How To Pass the 3 Hour Glucose Test While Pregnant
Two-Hour Glucose Test
The two-hour test requires a pregnant woman to drink 75 grams of oral glucose. You must be fasting for this test. Blood sugar levels are measured BEFORE drinking the Glucola, one hour after finishing and two hours after finishing.
Your blood glucose levels should be:
- Fasting: less than 92 mg/dL
- 1 hour after: less than 180 mg/dL
- 2 hours after: less than 153 mg/dL
Just ONE of these numbers above the cut off indicates gestational diabetes.
The International Association of Diabetes and Pregnancy Study Groups recommends the two-hour test.
Do I Have to Drink Glucola?
I’m in the minority of people who actually think the Glucola drink tastes good. I blame this on my unhealthy candy addiction.
However, because it is such a concentrated glucose solution, it can cause gastric irritation with nausea and vomiting in some women. Drinking it cold may help!
There are options for women who are unable to tolerate standard testing with the oral glucose drink. These include:
Serial Glucose Monitoring: Consists of a woman self-checking her blood sugar while fasting and at one or two-hour after meals over a period of time. Usually used for women at high-risk for GDM who cannot tolerate the oral glucose test.
Alternative Glucose Intake: Candy or even soda have been used instead of the Glucola drink. However, these methods appear to be less sensitive and have not been validated through large studies (2).
Intravenous Glucose Tolerance Testing: In rare cases, intravenous GTT can be used as an alternative but this approach has not been well validated (2).
Why Can’t They Just Test My A1c?
I’ve seen this posted in many pregnancy and parenting groups so I wanted to address it here.
The hemoglobin A1C test is a common way of diagnosing diabetes in non-pregnant women.
In simplest terms, this test measures the percentage of sugar attached to the hemoglobin protein found in your red blood cells. The red blood cells have an average lifespan of about 90-120 days. Therefore, the A1C test measures the average “sugar in your blood” for the past three to four months.
A normal A1C is less than 5.7%. A number between 5.7% to 6.4% indicates pre-diabetes. An A1C of over 6.5% is considered diabetes.
During pregnancy, red blood cell turnover increases. Basically, this means the red blood cell life span decreases and the body produces red blood cells at a more frequent rate.
Due to this, a pregnant woman’s A1C is probably slightly lower than if she were not pregnant. A1C is therefore not a good indicator of GDM.
Furthermore, the main concern with gestational diabetes is postprandial hyperglycemia, or, high blood sugar levels AFTER eating. The A1C test cannot accurately capture blood sugar levels after eating like the oral glucose test does.
The oral glucose tolerance test is currently the best and most standardized way to check for diabetes during pregnancy.

What If I Have Gestational Diabetes?
Most women diagnosed with gestational diabetes mellitus (GDM) will be able to control their blood sugars through lifestyle changes, mainly diet modification.
Monitoring your blood glucose levels at home is an important part of managing gestational diabetes. The general recommendation is to check blood sugar levels four times a day:
- when you wake up in the morning, before eating anything (fasting)
- 1-2 hours after breakfast
- then 1-2 hours after lunch
- and 1-2 hours after dinner
Your doctor should refer you to a registered dietitian nutritionist or diabetes educator who can help you learn how to deal with and manage GDM.
You may have to start insulin if blood sugar levels cannot be controlled through dietary modifications. Your doctor may decide to prescribe oral diabetic medications such as Metformin or glyburide but these DO cross the placenta.
Your OB/GYN may refer you to an endocrinologist who can help determine the best treatment for you.

Follow Up for Gestational Diabetes
After delivery, when the placenta is no longer producing hormones that affect the action of insulin, your blood glucose levels should return to normal. Sometimes, GDM can represent previously undiagnosed diabetes or pre-diabetes that you didn’t know about because you had never been tested before.
For this reason, it’s important to screen for diabetes between four to twelve weeks postpartum. Pregnancy-related changes or blood loss from delivery may still affect the A1C at this point. Therefore, most practices will use the oral glucose tolerance test again. In general, post-partum women will have the 75-gram oral GTT (the one-step test).
Women with a history of gestational diabetes are also at a higher risk of developing diabetes in the future. Therefore, if you’ve had GDM, you should get screened for diabetes regularly. Screening should be done at least every three years.
Gestational diabetes sounds scary and it can lead to serious complications if it is uncontrolled. Keep in mind that when you are monitoring and controlling your blood sugar levels, the risk of complications for you and your baby are greatly reduced.
If you are preparing to take the glucose tolerance test during your pregnancy, I hope this information was helpful! Feel free to leave any questions in the comments or let me know about your experience with the glucose tolerance test!
Related posts:
- How to Relieve Constipation During Pregnancy
- Hospital Bag Must-Haves for Pregnant Mamas
- Newborn Essentials (For The First 3 Months)
- Being Induced for Preeclampsia: My Labor Story
- What to Expect When Giving Birth During the COVID-19 Pandemic
Sources:
1. American Diabetes Association. 14. Management of diabetes in pregnancy: Standards of Medical Care in Diabetes—2020. Diabetes Care 2020;43(Suppl. 1):S183-S19. https://care.diabetesjournals.org/content/43/Supplement_1/S183
2. Durnwald, C. Diabetes mellitus in pregnancy: screening and diagnosis. Last updated Oct 29, 2019. From www.uptodate.com
